The Praxis Planner
your personal journal for us to work together
Your mental health journey is unique, and The Praxis Planner is your personalized space to explore it. Through guided reflections, exercises, and real-time feedback, this journal fosters collaboration between you and your care team. Whether tracking what’s working or identifying areas for adjustment, The Praxis Planner helps us tailor your care to truly fit your needs. Let’s work together to transform insight into action, and action into lasting change.

Our Journal
What is Patrescence: The Transition We Miss
We don’t talk enough about what actually happens to a man when he has a kid. It’s not just about “getting used to it.” It’s patrescence—the distinct, biological process of becoming a father. From remodeling neural pathways to shifts in stress hormones, a dad’s transformation is real, measurable, and essential to his child’s development. Let’s dive into the science behind the paternal identity shift and look at why treating fathers like backup caregivers is costing everyone.

Left on Read: Rejection Sensitivity and the ADHD Brain
When a patient with ADHD says “I know I’m overreacting, but I can’t stop,” they are not being dramatic. They are describing something neurobiologically real — a predictable consequence of dopaminergic prefrontal dysfunction interacting with the brain’s social pain circuitry. Rejection sensitivity is one of the most impactful features of ADHD and, in my experience, one of the most underaddressed in clinical training. This post on RSD covers what the research tells us about the underlying neuroscience, what it looks like when it walks into your office, and how to think about treatment when screening tools and symptom checklists have only told part of the story.

Matrescence: You’re Not Falling Apart. You’re Becoming.
There is a word for what happens to a woman when she becomes a mother—and it is not postpartum depression, not baby blues, not “the adjustment period.” It is matrescence: a developmental process as profound, disorienting, and biologically driven as adolescence, except that nobody talks about it the way they should. This post explores what the science now tells us about the maternal brain, the maternal body, and the maternal identity—and why having a name for this might be one of the most useful things we can offer the people living through it.
Therapists have the poetry, but prescribers need the math: what therapists should know about psychiatric medication.
Every week, therapists sit with clients who are on psychiatric medication — holding the most detailed, continuous picture of how that medication is actually going. They hear about the side effect that showed up in week two. They notice when the affect has gone flat in a way that feels different from the depression. They know about the ibuprofen for the back pain, the supplement someone started taking, the doses that got skipped during the work trip. And most of them have no idea what to do with any of it — not because they don’t care, but because nobody ever taught them that this information was clinically urgent, or how to move it across the treatment team in a way that actually changes care. This post is about that gap.
We need to be talking about weaning.
Weaning from breastfeeding is one of the most significant hormonal transitions a woman will experience in the postpartum period — and one of the least clinically supported. This post explores why the 3–6 month postpartum window, when most American mothers are weaning, is a period of compounding vulnerability: shifting reproductive hormones, the return of estrogen cycling and menstruation, postpartum thyroiditis (which affects 5–10% of postpartum women and often goes undetected), cumulative sleep deprivation, and the withdrawal of oxytocin and prolactin can converge into a perfect storm of mood disruption that is often more destabilizing than the early postpartum period itself. While breastfeeding is consistently associated with lower rates of postpartum depression, the direction of that relationship is complex — and the medical literature on post-weaning psychiatric symptoms remains startlingly thin, with only thirteen documented syndromes across six published case reports, even as thousands of women describe the same experience in online communities. Drawing from both personal experience and clinical practice, this post examines the neuroendocrine landscape of lactation and weaning, the emotional weight of ending a breastfeeding relationship, and what evidence-based treatment actually looks like — including interpersonal and cognitive behavioral therapy, SSRIs and other medications, psychosocial breastfeeding support, and the kind of compassionate, unhurried care this transition deserves. If you are experiencing mood changes, insomnia, or anxiety during or after weaning, this post is for you.

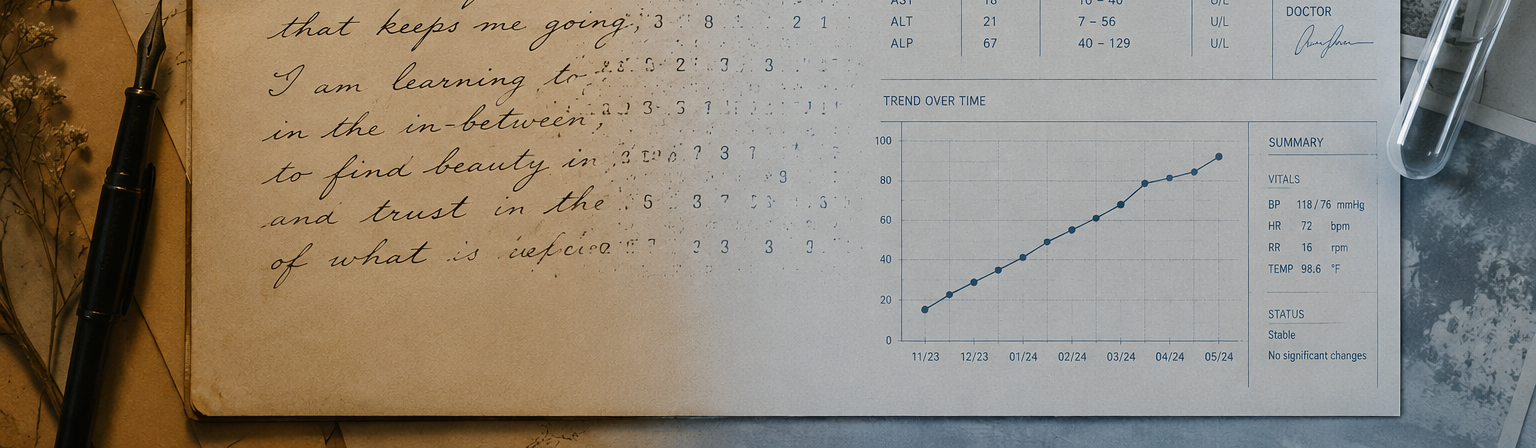
The Enduring Power of Pen and Paper: How Analog Practices Support Mental Health
This article highlights the enduring significance of analog practices—writing, doodling, drawing, and journaling—as essential tools for mental well-being, cognitive enhancement, and personal growth. Grounded in both historical tradition and modern neuroscience, these activities stimulate complex motor and cognitive processes that digital interactions often neglect. Research demonstrates that handwriting improves memory retention, promotes emotional regulation, and fosters mindfulness by slowing mental processes and grounding individuals in the present moment. Additionally, expressive writing and creative drawing serve as therapeutic outlets for processing emotions, reducing anxiety and depression, and supporting overall mental health. As part of a holistic approach to care, Praxis Mental Health encourages integrating these analog practices into both therapeutic work and personal wellness rituals, providing a much-needed counterbalance to the overstimulation of modern digital life.

The Praxis Standard: Elevating Mental Health Care Through Thoughtful, Integrated Mental Health Care
This article explores the Praxis Signature Framework, our model of elevated mental health care that integrates advanced psychiatric expertise with depth-oriented psychotherapy to deliver highly personalized, evidence-based treatment. Moving beyond routine medication management, we emphasize continuous reassessment, patient education, and shared decision-making to foster meaningful therapeutic progress. This journal entry highlights, through a case reflection, the importance of evaluating treatment effectiveness and discussing milestones in care. This entry underscores the need for clinicians to remain actively engaged in their patients’ mental health journeys. The Praxis Mental Health approach combines individualized, data-informed treatment plans with clear patient education and responsive support from the multidisciplinary team, including registered nurses. Our model exemplifies a higher standard of psychiatric and therapeutic care, aiming to empower patients and improve long-term outcomes through collaboration, curiosity, and compassionate care.

Being of Service to Mothers Means Listening First
This article explores the critical role of deep, attuned listening as the foundation for effective maternal mental health care. In a healthcare landscape that often prioritizes efficiency and symptom management, the act of slowing down to truly hear a mother’s story becomes a radical and transformative intervention. Drawing from psychodynamic principles, the author illustrates how emotions frequently labeled as pathological—such as anxiety, anger, or overwhelm—often carry deeper relational and existential meaning within the context of new motherhood. Through clinical reflection and personal experience, the piece underscores the importance of honoring the full emotional landscape of motherhood, including grief, joy, ambivalence, and vulnerability. By creating therapeutic spaces that foster emotional honesty and connection, providers can move beyond prescriptive checklists to develop more accurate, compassionate, and effective treatment plans. The author advocates for a model of care rooted in relational presence, where listening is not a passive act but an essential service that empowers mothers to feel seen, validated, and capable in their transition to motherhood.

Scholarship as a Form of Care: How Curiosity Shaped My Career
This narrative explores the author’s professional journey from licensed Marriage and Family Therapist to psychiatric nurse practitioner, illustrating how a foundation of curiosity and scholarship shaped a career devoted to integrative mental health care. Recognizing the limitations of a single-modality approach, the author pursued advanced training to bridge the gap between psychotherapy and psychiatry, blending relational insight with medical expertise. This career path exemplifies how ongoing scholarship—through the continuous study of neurobiology, pharmacology, and psychological research—can directly enhance patient care. Rather than viewing academic inquiry as separate from clinical work, the author describes how curiosity fuels a practice rooted in collaboration, education, and evidence-informed treatment. This model positions scholarship not as an academic exercise, but as an essential form of care that empowers patients through both understanding and meaningful therapeutic change.
